Table of content
Resistance training is the principal mode of exercise when it comes to improving muscle strength, power, and hypertrophy. Additionally, improving muscle strength, power, and hypertrophy coincides with improvements in the performance of many athletic tasks such as jumping, sprinting, and change of direction [1, 2]. Resistance training also plays an important role in injury prevention and rehabilitation and has numerous health benefits [3, 4, 5]. Therefore, it is no surprise that sports scientists, strength and conditioning coaches, sports coaches, physiotherapists, and fitness coaches highly emphasize resistance training within their overall training program when working with athletes, clients, or patients.
The traditional way of monitoring and prescribing resistance training
When designing a resistance training program, coaches typically consider several training variables such as the choice and order of the exercises, load, repetition range, volume, and rest, to name a few. According to the literature, training load and volume (i.e., what loads are you using and for how many sets and repetitions) are driving training adaptations the most [6, 7], so coaches often spend the greatest amount of time tailoring them to their athletes’ or clients’ needs.
How do we prescribe resistance training loads and volume? Let’s start with the loads. In principle, when working with your athletes or clients, you can guesstimate the “appropriate” loads for a given exercise. However, this likely won’t lead to any meaningful results over the long run, and it might even be dangerous in some circumstances. Therefore, to have greater control of the training program as a whole and individuals’ progress over time, coaches often evaluate their athletes’ or clients’ maximum strength capacity. Traditionally, the most popular way of establishing someone’s maximum strength consists of an incremental loading test whereby the loads are progressively increased until the maximum load that can be lifted only once is found. This so-called one-repetition maximum (1RM) is then used to derive percentages of maximum strength (i.e., sub-maximal loads) which further allows coaches to periodize the relative intensity of the training sessions to maximize adaptation and allow for recovery.
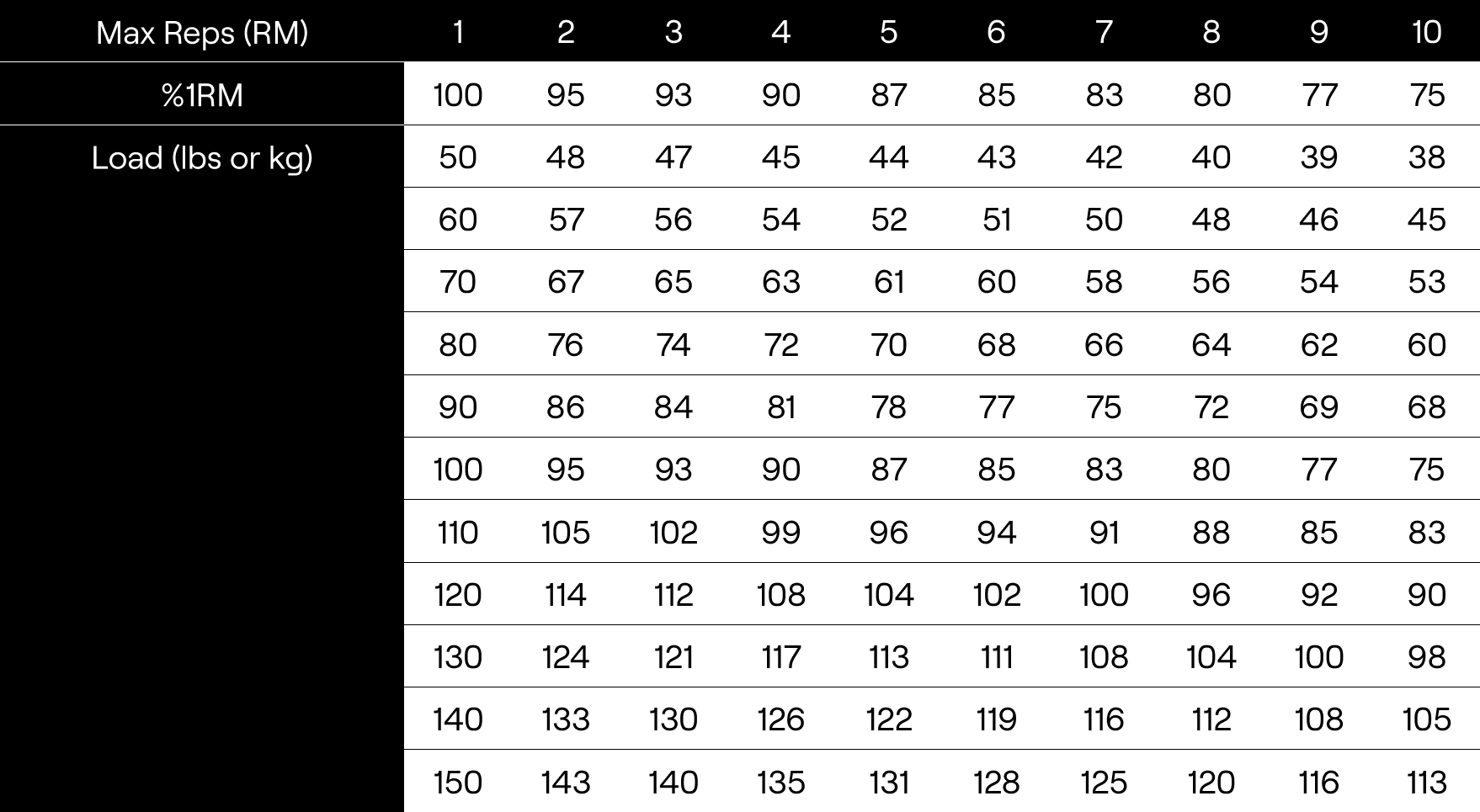
Now that we established the most common way of establishing someone’s strength capacity and how to prescribe relative loads based on it, let’s talk about volume. It is important to appreciate that there are different ways of monitoring resistance training volume. However, it is often defined as the number of sets and repetitions performed for a given exercise (locally) or the entire training session (more globally). How many sets we want to prescribe for our athletes or clients will depend upon many factors, and that requires an article by itself, but for now, let’s appreciate how coaches often prescribe the volume of each set during resistance training. Traditionally, set volume is prescribed using a fixed, predetermined number of repetitions within the set based on the theoretical relationship between a maximum number of repetitions individuals can do with a given percentage of 1RM (%1RM). Indeed, popular sports science and strength and conditioning textbooks [8] display this relationship in the tabular form which highlights how many repetitions one can do given the relative load they are using (e.g., a maximum of 10 repetitions can be performed with 75% of 1RM load). Armed with the information about their athletes’ or clients’ maximal strength capacities, coaches then periodize the relative loads and the amount of volume completed across training microcycles and macrocycles (or training blocks) in order to achieve the training goals. While this method of monitoring and prescribing resistance training has “worked” for decades (and it still “works”) for many coaches and their athletes and clients, it is far from optimal.
While the training periodization for different training goals is beyond the scope of this blog post, it is important to appreciate the flaws of the traditional way of monitoring and prescribing resistance training as described above. We will cover the two major ones.
The myths and flaws of the 1RM-based training method
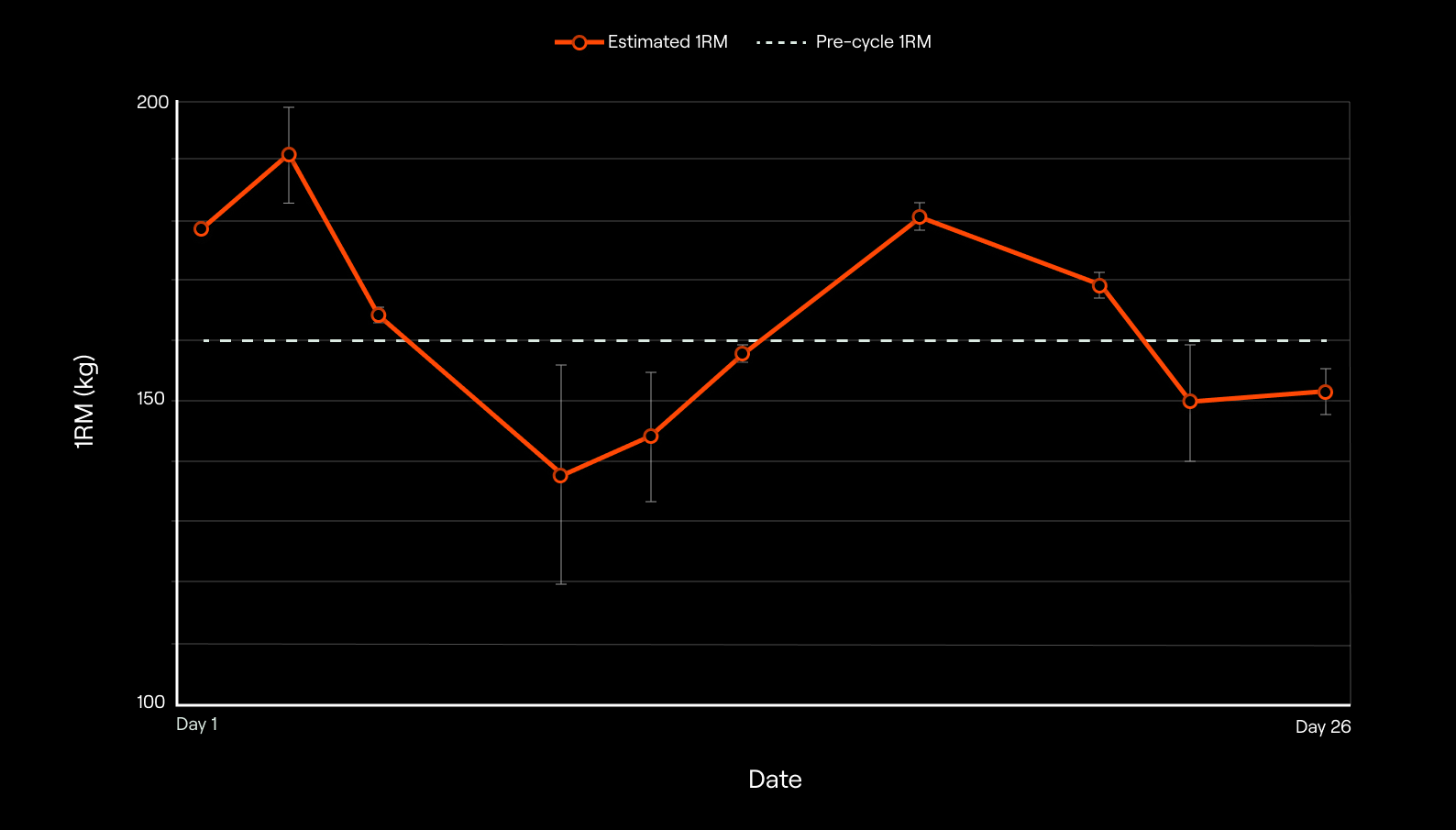
Firstly, establishing a 1RM for an athlete or a client takes time, usually about 30-60 minutes, depending on the person’s training status, number of attempts, rest periods, and so on. Not only that, every maximal test exposes individuals to an increased risk of injury, so doing them frequently is not ideal when working with athletes or clients [9]. However, the maximal strength capacities of individuals, as quantified via 1RM, can quickly become outdated as training adaptations occur [10]. Therefore, coaches can be left in a dilemma between testing 1RM more often so they can prescribe the loads more accurately (because they will match their athletes’ or clients’ current strength levels) and spending the time required for 1RM tests on other important things in the overall training plan. Even if the coach decides to re-evaluate the 1RM of their athletes and clients periodically, prescribing resistance training using the 1RM can under- or over-estimate individuals’ abilities on a given day due to normal day-to-day variability in readiness to train. Just think about it, how many times did you go to a gym, look at your own training, put the loads on the bar that your program called for, and then feel that it was easier or heavier than you’d expected it to be? Probably a lot of times. Nevertheless, you certainly don’t think that the load your program calls for is “just right” in every training session. Well, the same can be said for your athletes and clients when you’re prescribing them the loads based on their 1RM. This is especially relevant in sports in which athletes are exposed to other training outside the gym which complicates fatigue management. For instance, you’re having a gym session with your football team in the afternoon, but they also have a morning football session on the pitch due to a congested schedule. Your program calls for 5 x 3 with 85% of 1RM, but for most of your athletes, 85% is more like 90 or 95% today because they are tired from their morning session, and continuing with the workout would lead to overshooting (i.e., training harder than ideal). In this example, overshooting is especially important to avoid as we’re exposing our athletes to a greater risk of injury. The example we just saw doesn’t have to be so extreme, even though it often happens with congested schedules and in preparatory periods; A similar scenario can apply even if there is a day of complete rest between the sessions. Things can work the other way too. Let’s say that your client got a job in the firm he always wanted to work for, and he is super excited. He comes to the gym and starts working out using your program which again calls for 5 x 3 with 85 % of 1RM (note that there is nothing magical about this load, set, and rep scheme), but because your client is feeling extremely well, 85% feels more like 75% for him today, and continuing with the workout based on your original prescription would lead to undershooting (i.e., training less hard than ideal). There is a plethora of reasons why your daily readiness to train might fluctuate; just think about how many factors can affect your mood and training. The quality and quantity of sleep, personal and professional relationships, job or school, recovery rates, and nutrition to name a few, can all affect how well are you going to perform in the gym on a given day.
Secondly, the number of repetitions one can perform with a given %1RM has been shown to be highly individual and depends upon the exercises used and the training background of the individuals [11, 12]. This can be very problematic as prescribing the same relative load with a fixed number of repetitions will lead to heterogeneous training stimuli across individuals due to the potential differences in the level of effort experienced. Let’s unpack this a bit. Let’s say that you’re coaching Jane and Ana. Jane can do 15 repetitions with her 75% of 1RM, and Ana can do 11. However, the table from the textbook says that people will do 10 repetitions before they reach muscle failure with a load of 75% of 1RM. Considering this, you prescribe only 3 sets of 8 repetitions for both Jane and Ana. However, Jane and Ana likely won’t experience the same training stimulus because when they finish their sets, Jane will have 7 and Ana will have only 3 repetitions left in reserve, meaning that they are at different proximities to muscle failure. From the acute training response perspective, this can have implications for recovery between the workouts as Jane probably didn’t find her workout as challenging as Ana did. This is not a problem if it happens once or twice but imagine this scenario repeating every workout in a 12-week training block; the disparity in the training adaptations between Jane and Ana is inevitable even though they used “the same” training program. As before when we talked about under- and over-shooting, one can also expect that Jane and Ana will be able to do more repetitions with a given load as the training adaptations occur. Similarly, they might not perform as planned if their daily readiness to train doesn’t match the “predictions” of your training program. Either way, the error involved in our resistance training prescription can get very high which can lead to sub-optimal training adaptations in the long run.
Conclusion
Ok, you probably now realize the issues with the traditional resistance training monitoring and prescription approach. Please note that we covered only two fundamental ones related to this approach’s inability to account for daily readiness to train. There are many other shortcomings associated with this resistance training and prescription method which we might cover in the future. You might be asking yourself how to go about resistance training then; how to account for daily readiness to train and ensure that your athletes and clients are training appropriately during every workout. These are all great questions, and we will aim to cover all of them in the subsequent blog posts in the series, so stay tuned.
References
- Suchomel, T. J., Nimphius, S., & Stone, M. H. (2016). The importance of muscular strength in athletic performance. Sports Medicine, 46, 1419-1449.
- Suchomel, T. J., Nimphius, S., Bellon, C. R., & Stone, M. H. (2018). The importance of muscular strength: training considerations. Sports Medicine, 48, 765-785.
- Kraemer, W. J., Ratamess, N. A., & French, D. N. (2002). Resistance training for health and performance. Current Sports Medicine Reports, 1, 165-171.
- O’Connor, P. J., Herring, M. P., & Caravalho, A. (2010). Mental health benefits of strength training in adults. American Journal of Lifestyle Medicine, 4(5), 377-396.
- Feigenbaum, M. S., & Pollock, M. L. (1999). Prescription of resistance training for health and disease. Medicine and Science in Sports and Exercise, 31(1), 38-45.
- Kraemer, W. J., Ratamess, N. A., & French, D. N. (2002). Resistance training for health and performance. Current Sports Medicine Reports, 1, 165-171.
- Kraemer, W. J., & Ratamess, N. A. (2004). Fundamentals of resistance training: progression and exercise prescription. Medicine and Science in Sports and Exercise, 36(4), 674-688.
- Baechle, T. R., & Earle, R. W. (Eds.). (2008). Essentials of strength training and conditioning. Human kinetics.
- Niewiadomski, W., Laskowska, D., Gąsiorowska, A., Cybulski, G., Strasz, A., & Langfort, J. (2008). Determination and prediction of one repetition maximum (1RM): safety considerations. Journal of Human Kinetics, 19(2008), 109-120.
- Padulo, J., Mignogna, P., Mignardi, S., Tonni, F., & D’ottavio, S. (2012). Effect of different pushing speeds on bench press. International journal of sports medicine, 33(05), 376-380.
- Richens, B., & Cleather, D. J. (2014). The relationship between the number of repetitions performed at given intensities is different in endurance and strength trained athletes. Biology of Sport, 31(2), 157-161.
- Sanchez-Medina, L., & González-Badillo, J. J. (2011). Velocity loss as an indicator of neuromuscular fatigue during resistance training. Medicine and Science in Sports and Exercise, 43(9), 1725-1734.
- Jovanović, M., & Flanagan, E. P. (2014). Researched applications of velocity based strength training. J Aust Strength Cond, 22(2), 58-69.